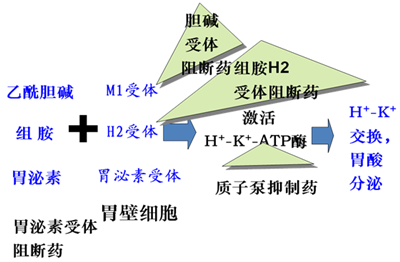
常用的對抗胃酸的藥物有三類,分別是:傳統(tǒng)的中和胃酸藥物、H2受體拮抗劑(H2RA)和質(zhì)子泵抑制劑(PPI)。后兩者通過抑制胃酸分泌來發(fā)揮抗酸的作用。
傳統(tǒng)的止酸劑對消化性潰瘍的療效不是很理想,H2RA出現(xiàn)于20世紀(jì)70年代,是酸相關(guān)性疾病治療上的里程碑,但仍然無法滿足全部的臨床需求,此后抑酸作用更強(qiáng)的PPI問世,使?jié)儾 ⑽甘彻芊戳鞑?GERD)的治愈率不斷提高[1]。
療效上,H2RA中,法莫替丁作用較強(qiáng),口服劑型在臨床較為常用,而PPI的抑酸作用強(qiáng)于法莫替丁[2, 3],因此對于消化道潰瘍[4, 5]、幽門螺桿菌[6, 7]患者療效更好,是治療這類疾病的一線治療藥物。對于預(yù)防和治療阿司匹林引起的消化道損傷,二者作用相似,PPI效果略好[8, 9]。因此,無論是預(yù)防還是治療應(yīng)用,PPI均作為用藥的選擇。
那么,H2受體拮抗劑的應(yīng)用價(jià)值何在呢?筆者總結(jié)以下幾點(diǎn):
1. PPI可能存在夜間酸突破(NAB)現(xiàn)象,即指應(yīng)用標(biāo)準(zhǔn)劑量PPI的患者在夜間(22 :00~6 :00)胃內(nèi)pH <4 .0且持續(xù)超過60 min的現(xiàn)象。這種現(xiàn)象不利于潰瘍愈合,除調(diào)整PPI治療方案外,睡前加服小劑量的H2RA可降低NAB的發(fā)生率[10]。
2.在PPI禁忌(如過敏)、經(jīng)濟(jì)條件不允許的時(shí)候,可考慮換用價(jià)格相對便宜的法莫替丁[11]。
3.因PPI抑酸作用很強(qiáng),長期應(yīng)用可能會導(dǎo)致高胃泌素血癥、維生素B12吸收障礙、低鎂血癥、骨質(zhì)疏松、骨折、小腸細(xì)菌過度增殖、獲得性肺炎等[12]。在預(yù)防性使用時(shí),對于高危患者可在抗血小板治療的前6個(gè)月聯(lián)合使用PPI,6個(gè)月后改為H2RA或間斷服用PPI[13]。
4.第4代H2RA羅沙替丁具有較西咪替丁、雷尼替丁和法莫替丁更好的療效和安全性,在抑制胃酸和治療潰瘍的療效方面與奧美拉唑、泮托拉唑相當(dāng)[14]。
此外,法莫替丁不與肝臟細(xì)胞色素P450酶作用,對于潛在藥物相互作用的情況,可考慮優(yōu)先使用。
補(bǔ)充:
1.消化道出血高危人群包括:年齡≥65歲,消化道潰瘍或出血病史,合并Hp感染,聯(lián)合或大劑量使用抗血小板藥、抗凝藥、NSAIDs、糖皮質(zhì)激素或SSRIs等藥物治療[15, 16]。
2.潰瘍同時(shí)合并幽門螺桿菌感染,應(yīng)先根除幽門螺桿菌,這樣可降低藥物致潰瘍的發(fā)生率。
References
[1]姚光弼.酸相關(guān)性疾病治療的前沿——從H_2受體拮抗劑到質(zhì)子泵抑制劑.中華消化雜志. 1999. (S1): 5-6.
[2] Tolbert K, Bissett S, King A, et al. Efficacy of oral famotidine and 2 omeprazole formulations for the control of intragastric pH in dogs. J Vet Intern Med. 2011. 25(1): 47-54.
[3] Shimatani T, Inoue M, Kuroiwa T, et al. Which has superior acid-suppressive effect, 10 mg omeprazole once daily or 20 mg famotidine twice daily? Effects of single or repeated administration in Japanese Helicobacter pylori-negative CYP2C19 extensive metabolizers. Dig Dis Sci. 2007. 52(2): 390-5.
[4] Tunis SR, Sheinhait IA, Schmid CH, Bishop DJ, Ross SD. Lansoprazole compared with histamine2-receptor antagonists in healing gastric ulcers: a meta-analysis. Clin Ther. 1997. 19(4): 743-57.
[5] Gisbert JP, González L, Calvet X, Roqué M, Gabriel R, Pajares JM. Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding peptic ulcer. Aliment Pharmacol Ther. 2001. 15(7): 917-26.
[6] Hu FL, Jia JC, Li YL, Yang GB. Comparison of H2-receptor antagonist- and proton-pump inhibitor-based triple regimens for the eradication of Helicobacter pylori in Chinese patients with gastritis or peptic ulcer. J Int Med Res. 2003. 31(6): 469-74.
[7] Scarpignato C. Antisecretory drugs, Helicobacter pylori infection and symptom relief in GORD: still an unexplored triangle. Dig Liver Dis. 2005. 37(7): 468-74.
[8] Chan FK, Kyaw M, Tanigawa T, et al. Similar Efficacy of Proton-Pump Inhibitors vs H2-Receptor Antagonists in Reducing Risk of Upper Gastrointestinal Bleeding or Ulcers in High-Risk Users of Low-Dose Aspirin. Gastroenterology. 2017. 152(1): 105-110.e1.
[9] Nema H, Kato M. Comparative study of therapeutic effects of PPI and H2RA on ulcers during continuous aspirin therapy. World J Gastroenterol. 2010. 16(42): 5342-6.
[10]李孝東,陳洪忠.質(zhì)子泵抑制劑的夜間酸突破及治療對策.藥學(xué)研究. 2013. 32(8): 487-489.
[11] Murakami K, Okimoto T, Kodama M, et al. Comparison of amoxicillin-metronidazole plus famotidine or lansoprazole for amoxicillin-clarithromycin-proton pump inhibitor treatment failures for Helicobacter pylori infection. Helicobacter. 2006. 11(5): 436-40.
[12] Chen J, Yuan YC, Leontiadis GI, Howden CW. Recent safety concerns with proton pump inhibitors. J Clin Gastroenterol. 2012. 46(2): 93-114.
[13]抗栓治療消化道損傷防治專家組.抗栓治療消化道損傷防治中國專家建議(2016·北京).中華內(nèi)科雜志. 2016. 55(7): 564-567.
[14]黃建權(quán),呂俊玲,胡欣.羅沙替丁醋酸酯藥理作用與臨床評價(jià).中國新藥雜志. 2014. 23(14): 1601-1605.
[15]抗血小板藥物消化道損傷的預(yù)防和治療中國專家共識組.抗血小板藥物消化道損傷的預(yù)防和治療中國專家共識(2012更新版).中華內(nèi)科雜志. 2013. 52(3): 264-270.
[16] Ahsberg K, H?glund P, Kim WH, von HCS. Impact of aspirin, NSAIDs, warfarin, corticosteroids and SSRIs on the site and outcome of non-variceal upper and lower gastrointestinal bleeding. Scand J Gastroenterol. 2010. 45(12): 1404-15.
(臨床藥師王楠)
|




